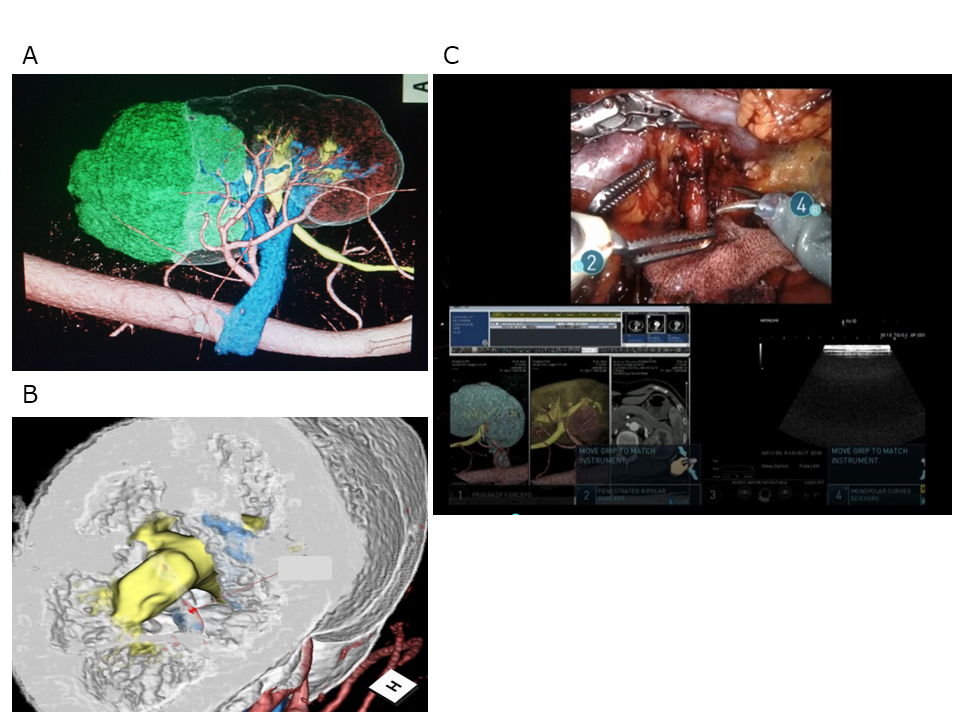
Introduction: Successful surgery in robot-assisted partial nephrectomy (RAPN), especially for highly complex tumors, relies on a detailed understanding of the anatomical relations of the tumor absolute and relative to the urinary tract and the vascular structures, including the renal pedicle. Intraoperative navigation with accurate information regarding tumor position relative to the surrounding urinary vascular structures undoubtedly assists the surgeon during RAPN. Methods: We retrospectively analyzed 323 patients who underwent RAPN using an ultra-high-resolution computed tomography (UHR-CT) scanner or area-detector CT (ADCT) to assess the perioperative and short-term functional outcomes of RAPN with intraoperative navigation using a UHR-CT scanner. Perioperative outcomes and the postoperative preservation ratio of estimated glomerular filtration rate (eGFR) were compared. Results: After the propensity score matching, we evaluated 99 patients in each group. Although the median warm ischemia time (WIT) was less than 25 min in both groups, it was significantly shorter in the UHR-CT group than in the ADCT group (15 min vs. 17 min, p = 0.032). Moreover, the estimated blood loss (EBL) was significantly lower in the UHR-CT group than in the ADCT group (33 mL vs. 50 mL, p = 0.028). However, there were no significant intergroup differences in the postoperative preservation ratio of eGFR at 3 or 6 months of follow-up (ADCT 91.8% vs. UHR-CT 93.5%, p = 0.195; and ADCT 91.7% vs. UHR-CT 94.0%, p = 0.160, respectively). Conclusions: Although no differences in short-term renal function were observed in intraoperative navigation for RAPN in this propensity score–matched cohort, this study is the first to demonstrate that UHR-CT resulted in a shorter WIT and lower EBL than ADCT. SOURCE OF Funding: None