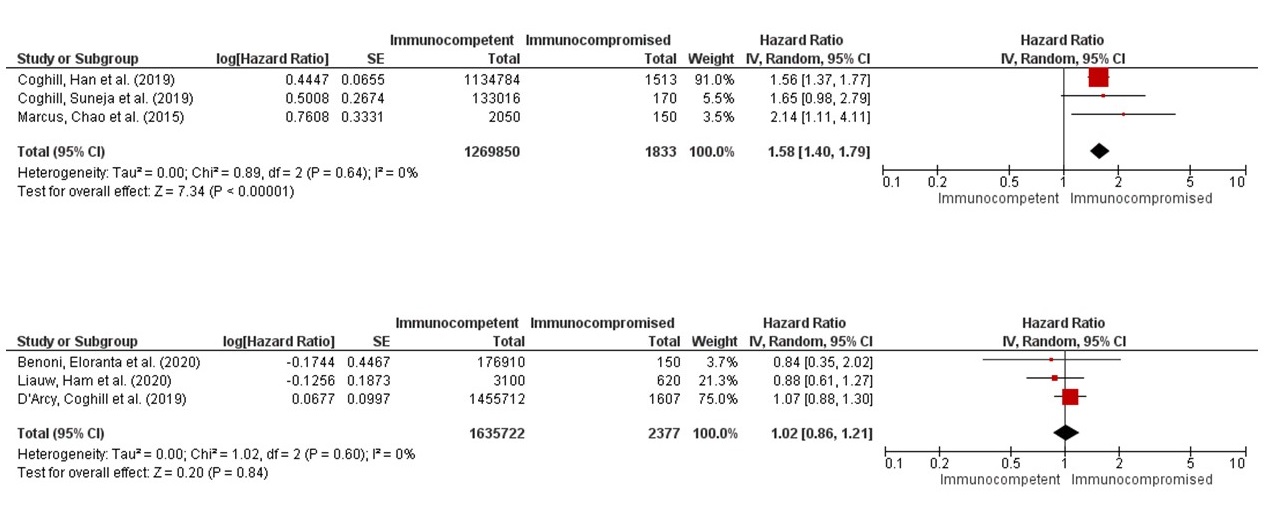
Introduction: To assess the oncological outcomes of immunocompromised vs immunocompetent prostate cancer (PCa) patients selected for active treatment. Methods: A systematic literature search was conducted from inception to July 2022 using PubMed/MEDLINE, Embase, and Web of Science databases (PROSPERO: CRD42022361504). Preferred Reporting Items for Systematic Reviews and Meta-analysis (PRISMA) guidelines were followed to identify eligible studies. The primary outcome consisted in assessing the cancer-specific mortality (CSM). Subgroup analyses of oncological outcomes have been performed according to the different immunodepression conditions. Results: Eighteen retrospective studies, including more than 3 million patients with localized or advanced PCa, met our inclusion criteria: nine studies for solid organ transplant (SOT), seven for HIV+, one for hematopoietic stem cells transplantation (HSCT) and one for rheumatoid arthritis (RA). Six studies provided an adjusted hazard ratio (HR) comparing CSM between immunocompetent and immunocompromised patients (3 for SOT and 3 for HIV), and a meta-analysis was then conducted. The forest plot (s. Fig1) did not show a statistical significant an overall higher risk of cancer-specific death in the immunocompromised patients (HR 1.28; 95% CI, 0.98-1.66; p=0.07; I2 74%). In the subgroup analysis restricted to HIV+ patients, immunocompromised patients showed higher CSM (HR 1.58; 95% CI, 1.40-1.79; p<0.001). Conversely, no difference was found for SOT patients (HR 1.02, 95% CI, 0.86-1.21; p=0.84). In the HSCT study, the standardized mortality-ratio was higher than primitive PCa in the general population, but the median overall survival was 10 or more years. In the AR study, the OS of PCa patients was lower in comparison with controls. Conclusions: Transplanted PCa patients seemed to present comparable oncological outcomes to those of the general population, despite a higher overall mortality in some series. Thus, it is advisable that treatment algorithm should be applied as by international guidelines for standard population. Other groups of immunocompromised PCa patients (HIV+ and RA) seemed to have a worse prognosis, so that more aggressive treatment modalities should be recommended. SOURCE OF Funding: None