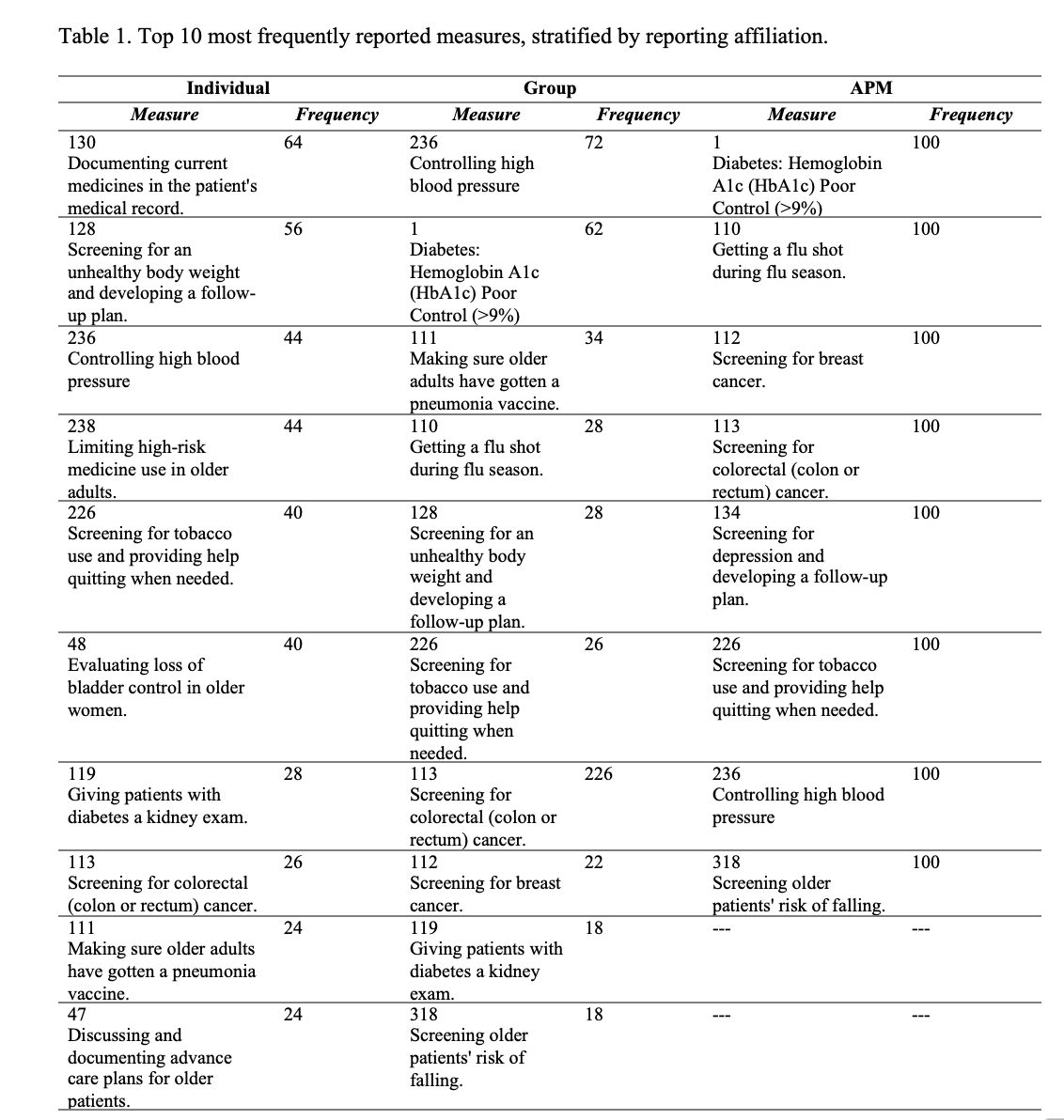
Introduction: The majority of urologists are required to participate in merit-based incentive payment system (MIPS) –a Medicare-mandate reporting system in which physicians must track and report quality measures. Medicare adjusts physician reimbursement based on performance across these measures, with the intention to improve the quality of patient care. However, very few MIPS measures are relevant to urology patients and it is unclear what measures urologists are choosing to track and report. Methods: We performed a cross-sectional analysis of MIPS measures reported by urologists for the most recent performance year. Urologists were categorized by their reporting affiliation (i.e., individual, group, or alternative payment model [APM]). We identified the measures which were most frequently reported by urologists. Among all measures reported, we identified those that were “topped out” (i.e., measures considered indiscriminate by Medicare because high performance is easily achieved) and those which were relevant for patients with urologic conditions (i.e., MIPS urology measures, qualified urologic registry measures, or those relevant to surgical care). Results: 8,297 urologists reported in MIPS during the 2020 performance year, of whom 14% reported as an individual, 56% as a part of a group, and 30% as part of an APM. Among the top 10 most frequently reported measures, none were specific for urologic care (Table 1). 65% of individual urologists, 58% of those in groups, and 92% in APMs reported at least 1 or more “topped out” measures. Only 11% of urologists reported measures that were directly relevant to patients with urologic conditions. Conclusions: Most measures reported by urologists are not directly relevant to patients with urologic conditions and remain a poor indicator of the quality of urologic care provided. As Medicare transitions MIPS to condition specific quality measures, it will be important for the urology community to develop and submit measures that will be most impactful for patients. SOURCE OF Funding: Avinash Maganty is supported by funding from the National Cancer Institute Ruth L. Kirschstein Postdoctoral Award F32 Grant F32 CA275021-01