Session: MP40: Prostate Cancer: Detection & Screening I
MP40-07: Has the introduction of multiparametric magnetic resonance imaging of the prostate and targeted biopsies led to a risk of overgrading of high risk prostate cancer? Results from a contemporary large multi-institutional series.
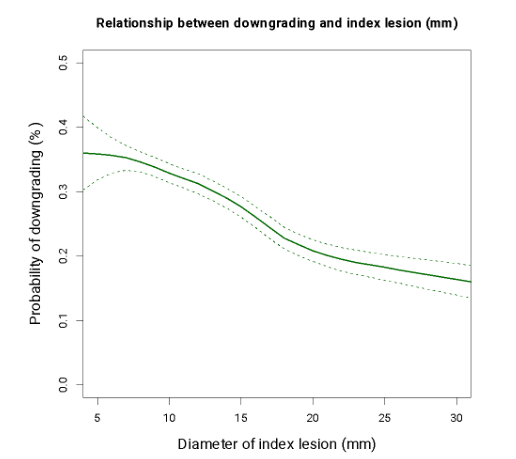
Introduction: Although multiparametric magnetic resonance imaging of the prostate (MRI) and mpMRI-targeted biopsies (TBx) are associated with improved disease assessment, concerns have been raised regarding the increased risk of PCa overgrading at TBx due to extremely accurate biopsy core deployment in the index lesion. We thus hypothesized that targeted biopsies are associated with a non-negligible risk of overgrading due to oversampling of the IL. Methods: We identified 403 men with localized PCa and GGG 4-5 who received MRI and subsequent systematic biopsy (SBx) plus TBx and eventually underwent RP at ten tertiary referral centers (2014-2021). The outcome was downgrading at RP (defined as GGG 1-3 at RP) of patients with GGG 4-5 at TBx only vs SBx only. Multivariable logistic regression models (MVA) were fitted. A local polynomial smoother weighted function was used to test the interaction between the rate of downgrading and clinical confounders. Results: Overall, 178 (44%) patients exhibited downgrading at RP. Specifically, 129 (32%) and 49 (12%) exhibited downgrading to GGG 3 and GGG 1-2, respectively. The rate of downgrading at RP of those men that had GGG 4-5 at SBx only vs TBx only vs TBx plus SBx was 25 (n=102) vs 30 (n=120), vs 13% (n=54), respectively (p=0.013). At MVA PCa with GGG 4-5 found at TBx was at higher risk of downgrading as compared to PCa with GGG 4-5 found at SBx (OR: 1.47). On the other hand, patients with higher GGG (OR: 0.29) and larger IL (OR:0.96) were less likely to exhibit downgrading (all p<0.05). At interaction analyses, the rate of downgrading was significantly associated with the size of the IL. Specifically, the probability of downgrading at RP decreased with increasing size of the IL, being roughly half for those with an IL size higher than 20 mm (Fig.). Conclusions: The rate of PCa downgrading at RP is higher in patients with GGG 4-5 detected at TBx only, as compared to both those with GGG 4-5 at SBx only and in both TBx and SBx. Patients with PCa with high GGG detected at TBx only should be carefully evaluated since they may harbor a more favorable disease and thus, they might benefit from a less intensive treatment approach. SOURCE OF Funding: None