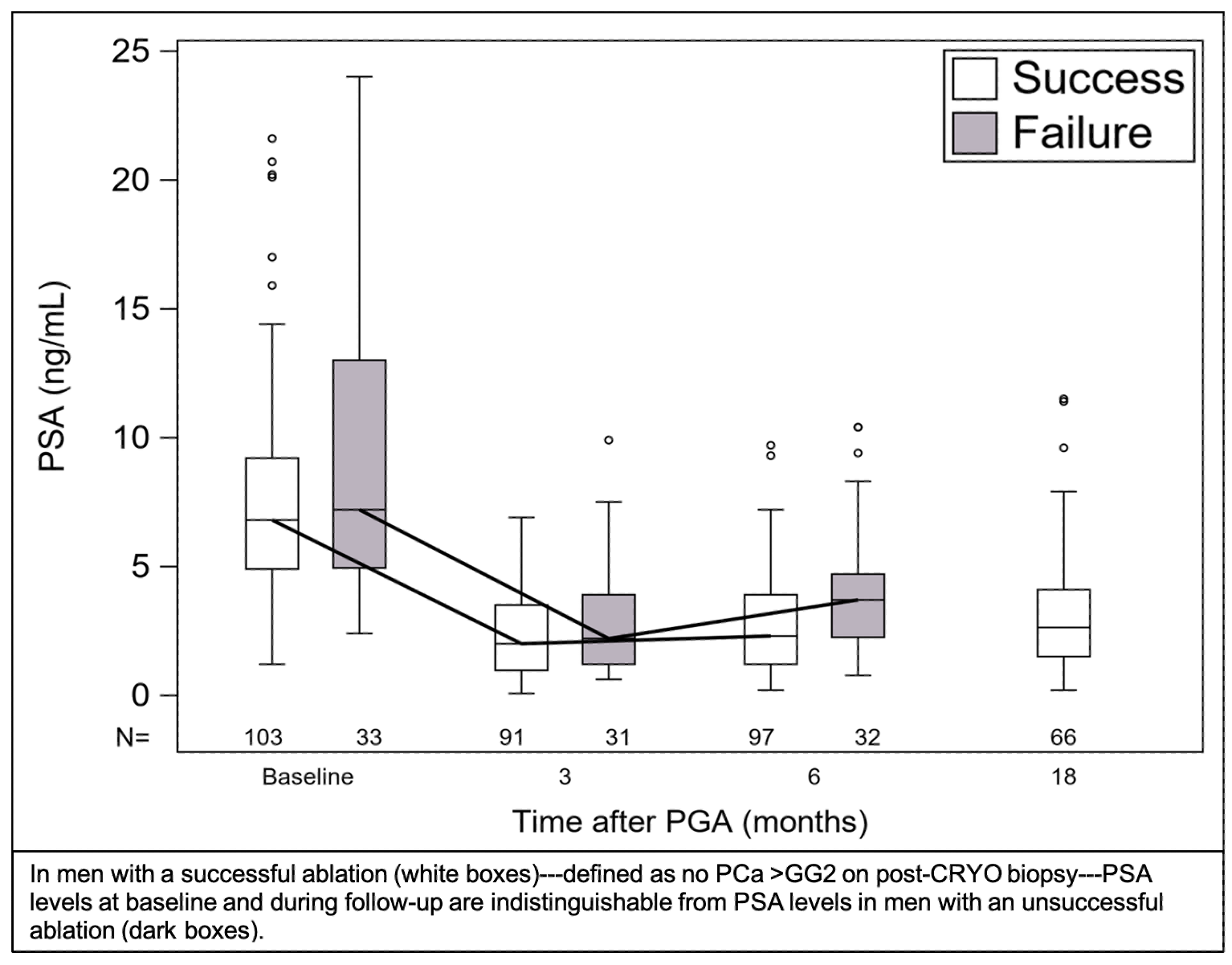
Introduction: We sought to determine the value of MRI and serum PSA levels in prediction of targeted biopsy results after partial gland ablation (PGA) of intermediate-risk prostate cancer (PCa) using cryotherapy (CRYO). Methods: In a prospective, observational trial (NCT03503643), 143 men with unilateral PCa (all >GG2) were enrolled. PSA and MRI-guided biopsy (MRGB) was performed before and after PGA with CRYO. CRYO treatment was a 2-cycle freeze of the affected prostate part using argon gas delivered via transperineal needles under image guidance. Participants underwent MRI/US fusion biopsy at baseline to determine eligibility; at 6 months to determine technical success; and at 18 months. Fusion MRGB in follow-up at 6 and 18 months employed tracking technology (JAMA Open: 31509206). Successful ablation = absence of PCa >GG2 on MRGB. Effects on urinary and sexual function were studied via EPIC-CP. Results: 95% of enrollees (136/143) completed f/u MRGB at 6 mo; 103 had a successful ablation (74%). Of the 103, 71 then had 18-mo f/u MRGB; success rate at 18 mo was 46/71 (65%); among 25 failures at 18 months, PCa was ipsilateral in 8, contralateral in 12, and bilateral in 5. Baseline MRI lesions (PIRADS >3) disappeared post-CRYO in 96/130 men (74%); PCa was found in 22/96 (23%) with no lesion and 11/34 (32%) with lesions (P=NS). In a mult-variate analysis, lesion diameter was the only parameter related to biopsy outcome. PSA levels were similar (p=NS) before and after CRYO in successful and failed treatments (FIGURE), as was PSA density. After CRYO, urinary function changed but little, or improved; overall sexual function decreased in 53/143 (39%), but only 10/143 men reported a severe decrement (>6 point decline). Conclusions: In the near to intermediate term, PGA with cryotherapy is a safe and moderately effective treatment of intermediate-risk PCa, when outcome is judged by MRGB. Neither PSA nor MRI, at baseline or during follow-up, appear reliable as indicators of post-treatment tissue findings. We postulate the treatment per se alters prostate anatomy and physiology in a manner that obscures a relationship between either test and pathological outcome. SOURCE OF Funding: This work was supported in part by the National Cancer Institute (R01CA195505), UCLA CTSI (UL1TR000124), the Jean Perkins Foundation, the Kent Kresa Family Foundation, and the Steven C. Gordon Family Foundation.