Session: MP59: Benign Prostatic Hyperplasia: Surgical Therapy & New Technology III
MP59-12: Can Anatomical Measurements on Preoperative Pelvic Magnetic Resonance Imaging Predict Postoperative Urinary Incontinence After Holmium Laser Enucleation of the Prostate?
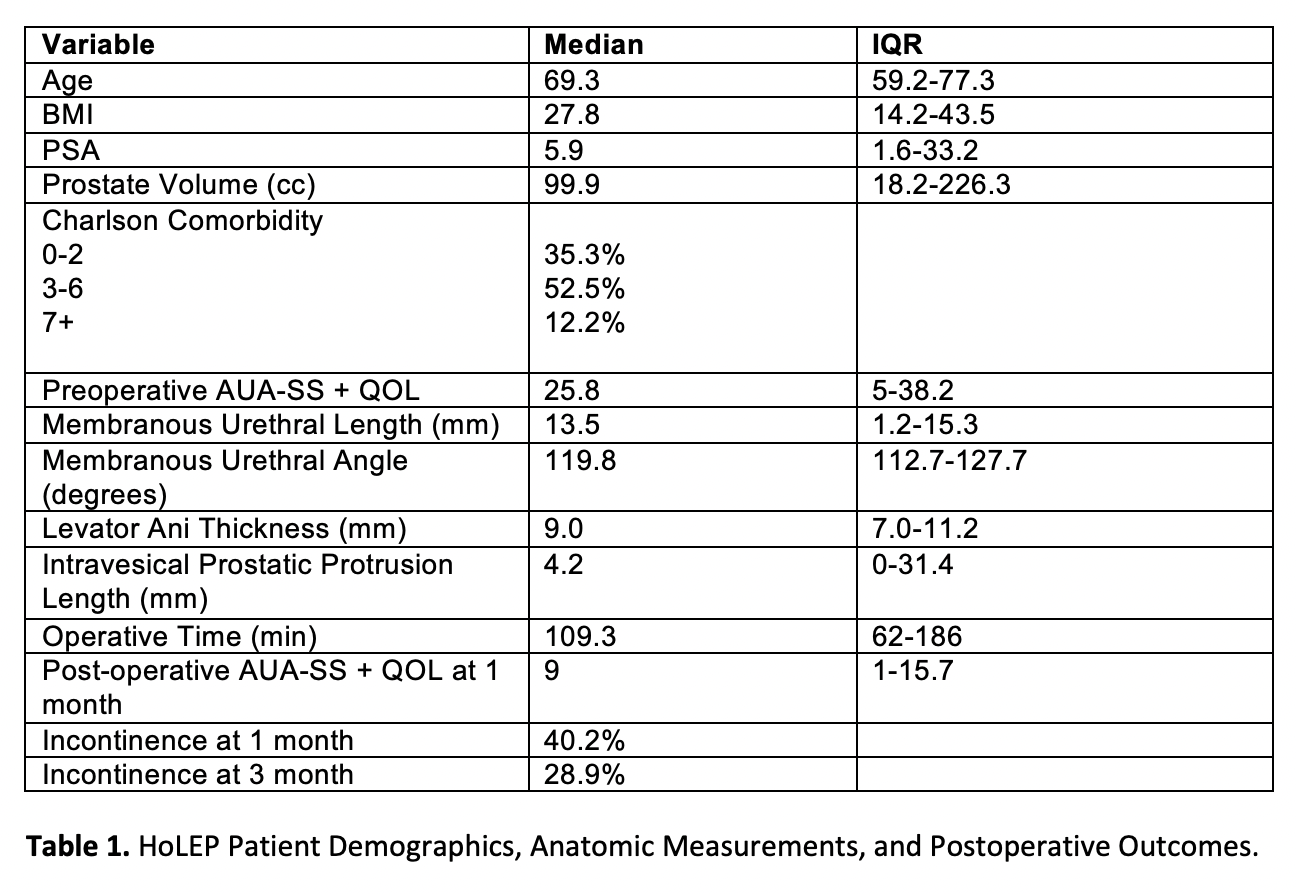
Introduction: Anatomical dimensions of the prostate and membranous urethra have been associated with urinary incontinence after robotic prostatectomy. However, such measures have not been extensively studied with regards to urinary incontinence after holmium laser enucleation of the prostate (HoLEP). Our objective was to assess the impact of preoperative measurements of membranous urethral length (MUL), membranous urethral angle (MUA), levator ani thickness (LAT), and intravesical prostatic protrusion length (IPPL) and whether they can be utilized to predict early postoperative urinary incontinence after HoLEP. Methods: We retrospectively reviewed our institutional HoLEP database for patients with available preoperative MRI pelvis/prostate from April 2019-June 2022. MRIs were analyzed for MUL (mm), MUA (degrees), LAT (mm), and IPPL (mm). Logistic regression analysis was performed defining urinary continence as <1 pad per day. Analysis was adjusted for age, body mass index, post-void residual, preoperative incontinence, and prostate-specific antigen (PSA). Separate analyses were performed using MUL, MUA, LAT, and IPPL. Results: 128 patients were identified with preoperative MRIs that underwent HoLEP (Table 1). The median age was 69.3 (59.2-77.3) and median preoperative PSA of 5.9 (1.6-33.2). At 1 month, MUL, MUA, LAT, and IPPL were not found to be significantly associated with incontinence (p=0.31, 0.45, 0.27, and 0.86, respectively). Similarly, at 3 months, MUL, MUA, and LAT were not associated with incontinence (p=0.66, 0.42, 0.31, respectively). However, IPPL was found to be associated with urinary incontinence at 3 months (OR=1.09 [1.01-1.29] p =0.049). Conclusions: Preoperative measurement of IPPL is associated with postoperative urinary incontinence after HoLEP. Further anatomic features such as MUL, MUA, and LAT, which have been associated with incontinence after robotic prostatectomy, do not have an effect on postoperative incontinence after HoLEP in our study, suggesting such anatomical variations may play less of a role in postoperative incontinence. Further studies are needed to assess the impact of anatomical dimensions on surgical outcomes after HoLEP. SOURCE OF Funding: None