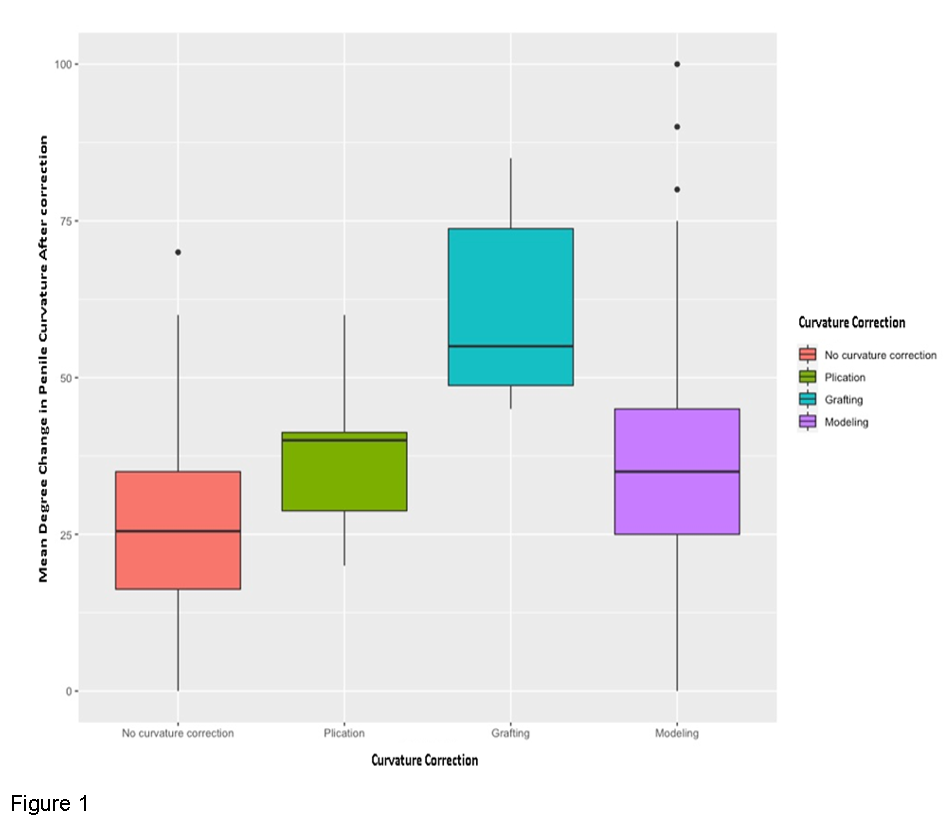
Introduction: Inflatable penile prosthesis (IPP) insertion is recommended for the treatment of patients with Peyronie’s Disease (PD) and significant erectile dysfunction (ED). Adjunctive procedures such as modeling, plication, or incision/excision and grafting can be used when there is residual curvature after IPP placement. We evaluated the management of curvature correction in patients with PD undergoing IPP among high-volume prosthetic urologists. Methods: We performed a retrospective study of 499 patients diagnosed with PD undergoing IPP by 10 high volume penile prosthetic surgeons. Demographic, intraoperative, and postoperative data were collected and analyzed. Results: 499 patients were included with mean age of 61.5 years (SD=10) and a median follow-up of 13.1 months (0-58.5 months). The mean preoperative curvature was 39.4° (SD=17.8) with dorsal curvature being the most common. Overall, 88 (17.6%) patients had IPP only with no adjunctive curvature correction procedure, 24 (4.8%) underwent plication, 10 (2.0%) underwent grafting, and 373 (74.7%) underwent modeling. Preoperatively, the mean starting curvature was 38.2° for the IPP-only group, 48.1° for the plication group, 60.6° for the grafting group, and 38.7° for the modeling group, p<0.001. Patients undergoing grafting had significantly fewer comorbidities: 1 (10%) had diabetes, none were smokers or had cardiovascular disease, p<0.001. After penile curvature correction, the mean curvature change was 30.0° for IPP-only group, 40.0° for plication group, 55.0° for grafting group, and 35.0° for the modeling group, p <0.001 (Figure1). Intraoperative complications occurred in 5 (1%) patients. Post-operatively, there were 43 (14.30%) non-infectious and 11 (2.20%) infectious complications. No significant difference in complications between groups. Conclusions: Although incision/excision and grafting seem to provide the greatest penile curvature correction for PD patients undergoing IPP placement, this adjunctive correction procedure is less commonly performed among high volume prosthetic urologists. Our results suggest grafting is reserved for patients with greater preoperative curvature and fewer preoperative comorbidities. SOURCE OF Funding: None