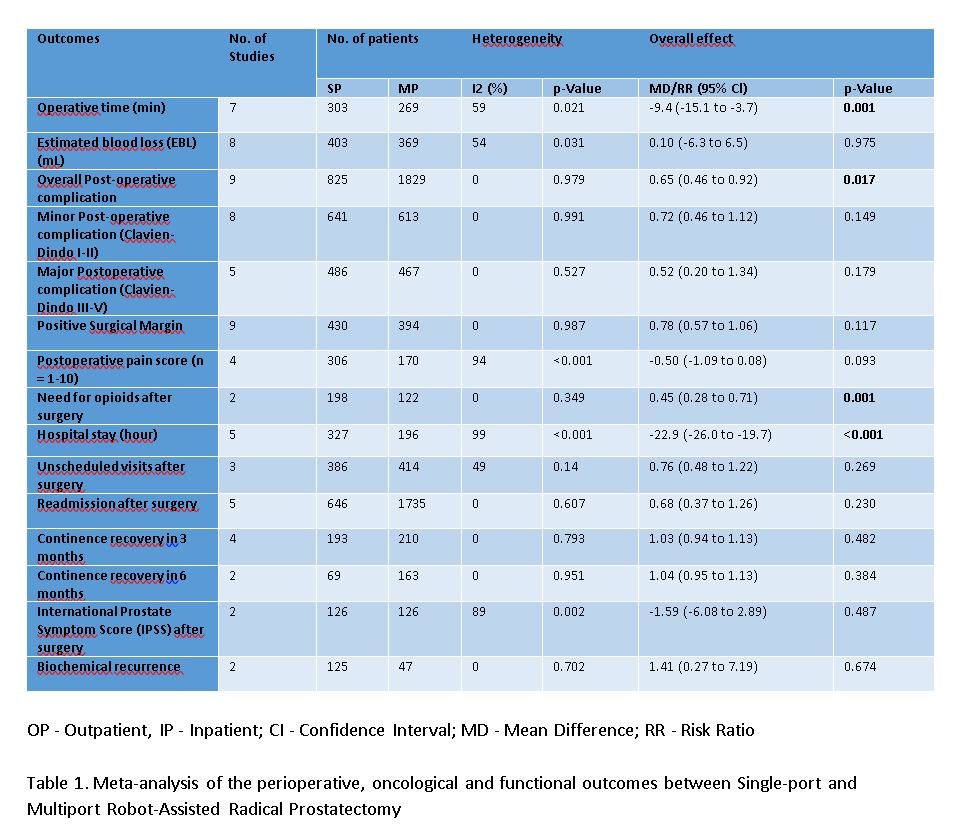
Introduction: Several institutions have reported their experience with outpatient robot-assisted radical prostatectomy (O-RARP). However, it is unclear if utilization of this approach represents an improvement over inpatient robot-assisted radical prostatectomy (I-RARP). This meta-analysis sought to compare the surgical outcomes between O-RARP and I-RARP. Methods: For relevant articles, three electronic databases, including PubMed, Scopus, and Web of Science, were searched from their inception until April 30, 2022. A meta-analysis has been reported in line with PRISMA 2020 and AMSTAR Guidelines. The risk ratio (RR) and weighted mean difference (MD) were applied for the comparison of dichotomous and continuous variables with 95% confidence intervals (CI). Results: Of the 297 retrieved abstracts, 12 underwent full-text review, and 11 studies were included in the final analysis, comprising a total cohort of 2,875 cases of robot-assisted radical prostatectomy (892 O-RARP cases and 1,983 I-RARP cases). Compared to I-RARP, the O-RARP group had lower mean operative time (MD = -9.4 minutes, 95% CI -15.1 to -3.7, 0.001), fewer overall post-operative complications (RR = 0.65, 95% CI 0.46 to 0.92, p=0.017), shorter hospital stay (MD = -22.9 hours, 95% CI -26.0 to -19.7, p= <0.001), and lower postoperative opioid requirements (RR = 0.45, 95% CI 0.28 to 0.71, p=0.001). There were no significant differences in other outcomes, including: estimated blood loss, postoperative pain score, unscheduled visits after surgery, positive surgical margins, biochemical recurrence, International Prostate Symptom Score (IPSS) after surgery, or three- and six-month continence rates. (Table 1) Conclusions: This meta-analysis demonstrates that O-RARP is a safe and feasible option for patients undergoing surgery for localized prostate cancer. Further studies are needed to better evaluate optimal patient selection, associated healthcare costs, and patient reported outcomes. SOURCE OF Funding: None