(CS-116) Cod Fish Skin Graft (CFSG) Use in Early Reconstruction After Radical Excision of Infected Wounds is Safe and Effective
Co-Author(s):
Introduction: It is general practice to excise infected wounds like necrotizing soft tissue infection (NSTI), pyoderma gangrenosum and stage III hidradenitis suppurativa (HS) in stages during the first hospitalization. Patients are then given several weeks to months, typically in a long term care facility, for the wound to stabilize/fill in before definitive reconstruction. Due to the antimicrobial and anti-inflammatory nature of CFSG, we begin reconstruction during the first hospitalization in order to decrease deconditioning due to immobility and protein leak from large wounds, to decrease time away from work, and to improve quality of life. (1,2)
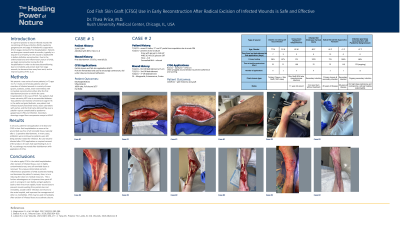
Methods: We present a case series of seven patients (n=7) ages 31-73, 3 male and 4 female patients who had resection of infected wounds in a variety of areas (groins, buttocks, axillas, lower extremities) with immediate reconstruction either after the first debridement/excision or within the same hospitalization in the case of NSTI. Two patients had lower extremity NSTI due to uncontrolled diabetes. Two patients had resection of extensive stage III HS in the axilla and groin/buttocks, one patient had infected acutely worsened venous stasis ulcerations with eschar, and the final had a dehisced flap over a patellar rupture complicated by pyoderma gangrenosum (PG) and infection. Secondary dressings ranged from compression wraps to NPWT.
Results: In all cases, patients had application of at least one CFSG in their first hospitalization as soon as the wound bed was free of all nonviable tissue, typically after 1-2 operative debridements. In many cases, antibiotics were continued as patients were still being actively treated for infection. No case became infected after CFSG application or required removal of the product. All cases had rapid healing (3,4). In PG, no pathergy was noted after debridement with application of CFSG.
Discussion: It is safe to apply CFSG in the initial hospitalization after excision of infected tissue, even in highly contaminated areas, once all nonviable tissue is removed. The unique antimicrobial and anti-inflammatory properties of CFSG accelerates healing and decreases the patient’s recovery time, in turn reducing the strain on medical resources. This is further advantageous as it improves time spent off work in a long-term care facility and gets patients back to their lives more rapidly. Faster wound closure prevents muscle wasting from protein loss and immobility, avoids further infection and returns to the acute hospital, and improves the management of other co-morbidities. CFSG may be used immediately after excision of infected tissue to accelerate closure.
Trademarked Items:
References: 1. Magnusson S, et al. Mil Med. 2017;182(S1):383-388. 2. Badois N, et al. J Wound Care. 2019;28(9):624-628. 3. Lullove EJ, et al. Wounds. 2021;33(7):169–177. 4. Yang CK, Polanco TO, Lantis JC 2nd. Wounds. 2016;28(4):112-8.

.png)