
Poster Session C
Pediatric autoimmune diseases: Kawasaki disease, juvenile dermatomyositis and juvenile localized scleroderma

Leigh Stubbs, MD, MPH
Baylor College of Medicine
Houston, TX, United States
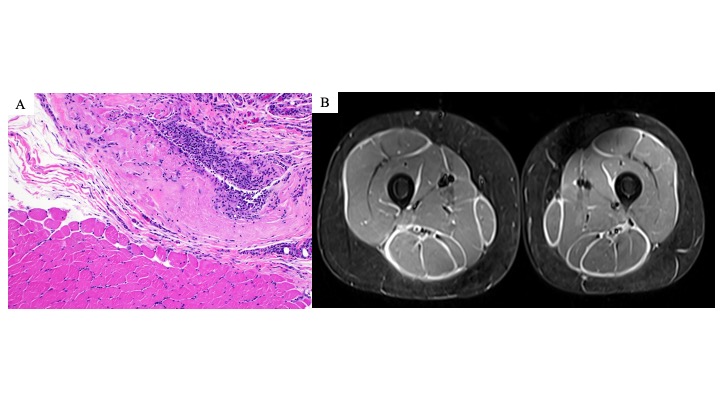 Figure 1. Examples of eosinophilic fasciitis pathology and MRI findings. (A) Left lower leg muscle and fascia biopsy from patient 4 consistent with eosinophilic fasciitis. Hematoxylin and eosin (H &E) section (magnification, x100) showing fascia with underlying muscle. The fascia shows thickening and inflammatory cell infiltration (many macrophages and lymphocytes, few plasma cells, and rare eosinophils). (B) MRI bilateral thighs with and without contrast of patient 4 demonstrating extensive, symmetric fasciitis on STIR axial image.
Figure 1. Examples of eosinophilic fasciitis pathology and MRI findings. (A) Left lower leg muscle and fascia biopsy from patient 4 consistent with eosinophilic fasciitis. Hematoxylin and eosin (H &E) section (magnification, x100) showing fascia with underlying muscle. The fascia shows thickening and inflammatory cell infiltration (many macrophages and lymphocytes, few plasma cells, and rare eosinophils). (B) MRI bilateral thighs with and without contrast of patient 4 demonstrating extensive, symmetric fasciitis on STIR axial image. 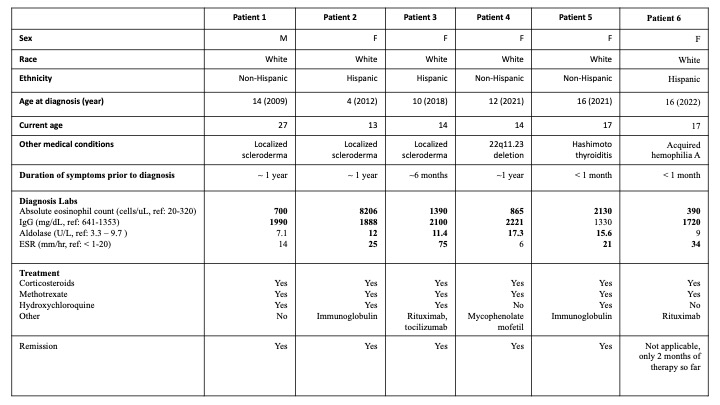 Table 1. Juvenile eosinophilic fasciitis cohort patient characteristics. Bolded laboratory values are elevated above reference ranges.
Table 1. Juvenile eosinophilic fasciitis cohort patient characteristics. Bolded laboratory values are elevated above reference ranges.  Figure 2. Positive prayer sign at initial presentation in juvenile eosinophilic fasciitis. Here are examples of patients 3, 4, 5, and 6 demonstrating a positive prayer sign at the initial diagnosis. The prayer sign is due to skin induration and fascial fibrosis leading to joint contractures and tendon retraction.
Figure 2. Positive prayer sign at initial presentation in juvenile eosinophilic fasciitis. Here are examples of patients 3, 4, 5, and 6 demonstrating a positive prayer sign at the initial diagnosis. The prayer sign is due to skin induration and fascial fibrosis leading to joint contractures and tendon retraction.