
Poster Session C
Fibrosing rheumatic diseases (scleroderma, MCTD, IgG4-related disease, scleroderma mimics)

Michael Hughes, PhD, MBBS, BSc, MSc, MRCP
Tameside and Glossop Integrated NHS Foundation Trust & The University of Manchester
Manchester, United Kingdom
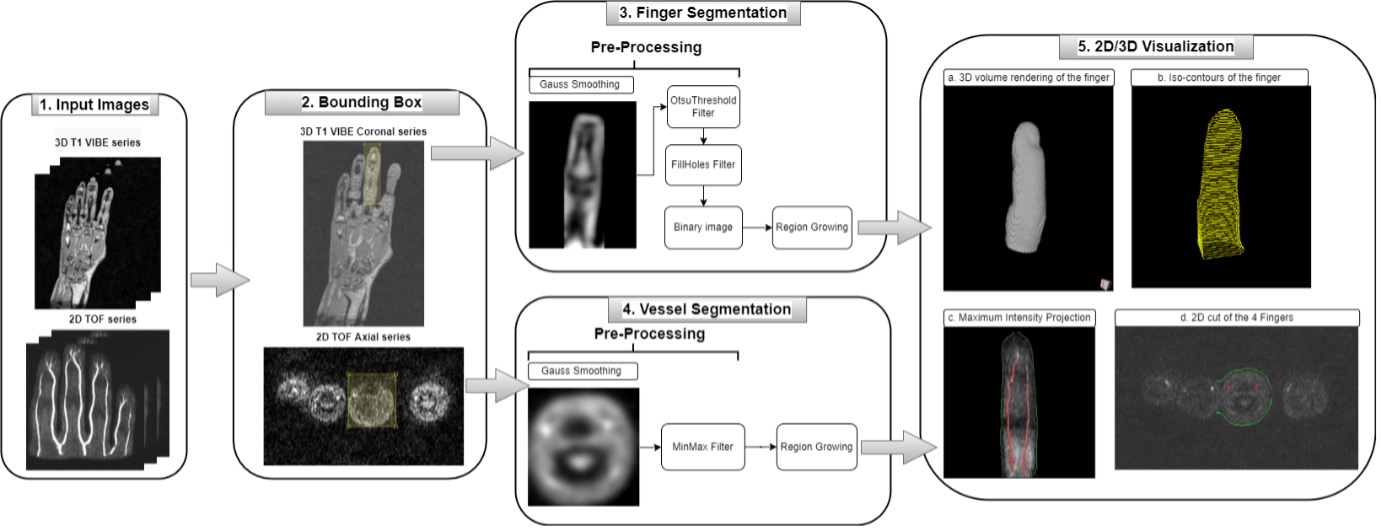 Figure 1. Workflow of the finger and vessel segmentation. DYNAMIKA (IAG, Image Analysis Group) workflow. Left-sided images: 3D T1 VIBE images and 2D TOF images are uploaded. The target finger is identified and outlined with a bounding box. Middle images: Finger segmentation model applied to generate the volume of the finger and the vessels segmentation model is applied to generate the vessels volume. Right-sided images: 3D rendering of the segmented finger and blood vessels.
Figure 1. Workflow of the finger and vessel segmentation. DYNAMIKA (IAG, Image Analysis Group) workflow. Left-sided images: 3D T1 VIBE images and 2D TOF images are uploaded. The target finger is identified and outlined with a bounding box. Middle images: Finger segmentation model applied to generate the volume of the finger and the vessels segmentation model is applied to generate the vessels volume. Right-sided images: 3D rendering of the segmented finger and blood vessels.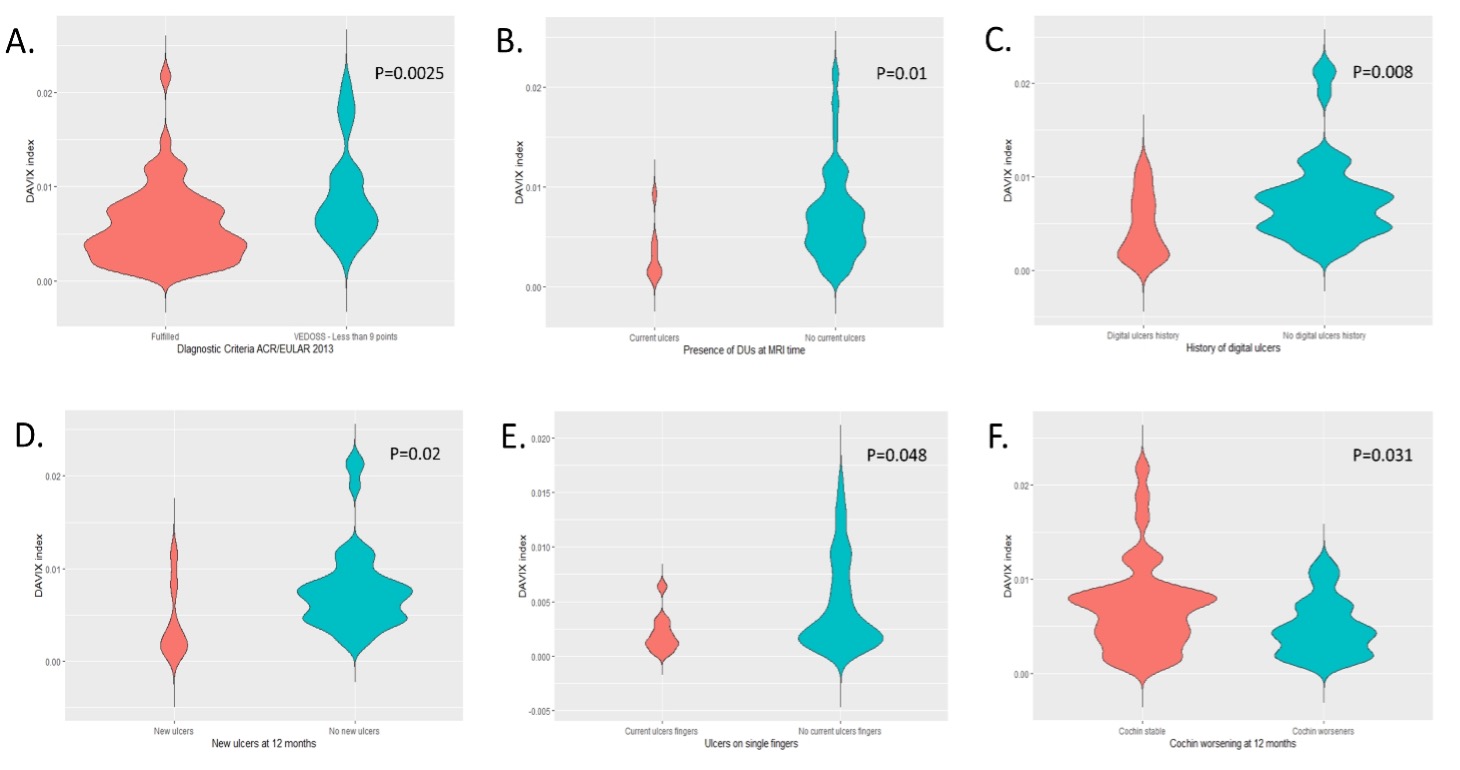 Figure 2. DAVIX in patients who fulfilled the ACR/EULAR 2013 SSc classification criteria versus patients presenting a score < 9 i.e., very early diagnosis of SSc (VEDOSS) (A). DAVIX in patients with baseline digital ulcers versus patients without baseline digital ulcers (B). DAVIX in patients with history of digital ulcers versus patients who never experienced digital ulcers disease (C). DAVIX in patients without baseline digital ulcers who developed digital ulcers at 12-month follow up versus patients without baseline digital ulcers who did not develop new ulcers after 12 months (D). DAVIX of the single fingers of the dominant hands of patients presenting with at least one digital ulcer at baseline: fingers with current ulceration vs fingers without current ulceration (E). DAVIX in patients presenting a stable CHF at 12-month follow up vs patients experiencing a worsening in the CHF after 12 months (F).
Figure 2. DAVIX in patients who fulfilled the ACR/EULAR 2013 SSc classification criteria versus patients presenting a score < 9 i.e., very early diagnosis of SSc (VEDOSS) (A). DAVIX in patients with baseline digital ulcers versus patients without baseline digital ulcers (B). DAVIX in patients with history of digital ulcers versus patients who never experienced digital ulcers disease (C). DAVIX in patients without baseline digital ulcers who developed digital ulcers at 12-month follow up versus patients without baseline digital ulcers who did not develop new ulcers after 12 months (D). DAVIX of the single fingers of the dominant hands of patients presenting with at least one digital ulcer at baseline: fingers with current ulceration vs fingers without current ulceration (E). DAVIX in patients presenting a stable CHF at 12-month follow up vs patients experiencing a worsening in the CHF after 12 months (F).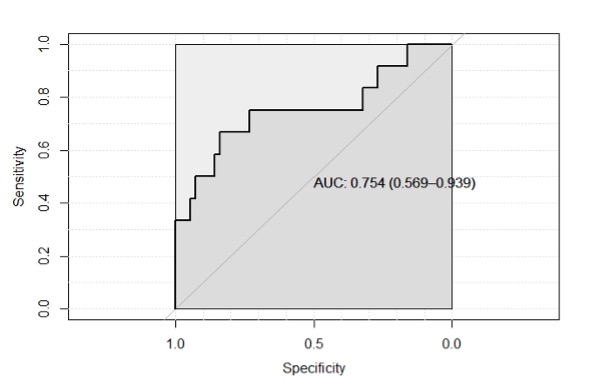 Figure 3. ROC curve with area under curve for the performance of the DAVIX index in the detection of new digital ulcers at 12 months. The 0.36% cut-off shows a specificity of 84% and a sensitivity of 67% in identifying patients who went on developing new digital ulcers. Patients with a dominant hand DAVIX © index inferior to 0.36% showed a significantly higher risk of developing new ulcers at 12 months (Incident Risk Ratio=4.55, Odds Ratio=7.31, Attributable fraction in the exposed=78%, P=0.005).
Figure 3. ROC curve with area under curve for the performance of the DAVIX index in the detection of new digital ulcers at 12 months. The 0.36% cut-off shows a specificity of 84% and a sensitivity of 67% in identifying patients who went on developing new digital ulcers. Patients with a dominant hand DAVIX © index inferior to 0.36% showed a significantly higher risk of developing new ulcers at 12 months (Incident Risk Ratio=4.55, Odds Ratio=7.31, Attributable fraction in the exposed=78%, P=0.005).