
.png)
Sedation

Ezra B. Goldberg-O'Neil, DDS
Pediatric Dental Resident
University at Buffalo/Women and Children’s Hospital of Buffalo, Buffalo, NY
The University at Buffalo
Buffalo, New York, United States

Kathleen M. Rusnak, DDS
Pediatric Dental Resident
University at Buffalo/Women and Children’s Hospital of Buffalo, Buffalo, NY
University at Buffalo
South Wales, New York, United States
Allana Langen, Bachelor's of Science, Sociology and English
University Pediatric Dentistry

Christopher Heard, MD
Attending Anesthesiologist
University at Buffalo
Buffalo, New York, United States
Carrie Wanamaker, DDS, DDS
Program Director, Advanced Education in Pediatric Dentistry
University at Buffalo
Buffalo, New York, United States
Assessment of the Traffic Light Model for Pediatric Sedation Dentistry, Heard C, Rusnak K, Langen AM, Goldberg-O’Neil E, (University at Buffalo, Buffalo, New York) Research supported by University Pediatric Dentistry Current data confirm the utility of the Traffic Light Airway model, though may imply that continued chin lift should be changed from a Yellow Light event to a Green Light event. During deep sedation procedures, necessity for airway management interventions was common. Deep sedation requires careful monitoring of the patient’s airway and the clinical skill-set to manage airway interventions.
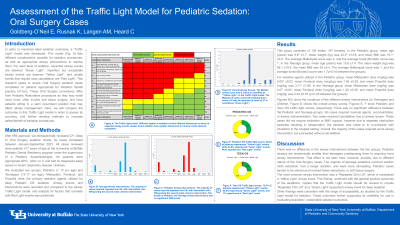
Purpose: This research evaluates if the novel Airway Traffic Light model developed by Dr. Christopher Heard accurately reflects airway complications and interventions for pediatric patients undergoing deep intravenous sedation. In this model, Red Light is an unsafe airway event requiring cancellation of the procedure, Yellow Light includes conditions which are imperfect, but safe to proceed, and Green Light are routine conditions.
Methods: University at Buffalo’s Institutional Review Board approved this ongoing retrospective chart review, which investigates sedation procedures performed between January and September of 2021 on patients under 18 years of age. Airway scores and interventions are being compared to the Airway Traffic Light model, and analysis for factors that correlate with Red Light events will be performed. Chi squared analysis will be used to compare the rates of Red Light events between sedation types.
Results: To date, 271 charts have been reviewed. The median behavior score was 9 (ranging between 7 and 10), and the median airway score was 6 (ranging between 1 and 10). 34% of pediatric patients/26% of teen patients were Green Light, 66% of pediatric patients/72% of teen patients were Yellow Light, and zero pediatric patients had Red Light Airway events while 1% of teen patients did. No cases required reversal agents, succinylcholine, airway instrumentation. 2 required cancellation. The majority of the cases required some airway intervention, but proceeded without cancellation.
Conclusion: