
.png)
Growth & Development

Jacob J. Altmire, DDS
Pediatric Dental Resident
University of Rochester, Rochester, NY
Eastman Institute for Oral Health
Webster, New York, United States
Ritu Shah, DMD
Research Mentor
University of Rochester
Rochester, New York, United States
Ritu Shah, DMD
Research Mentor
University of Rochester
Rochester, New York, United States
Cynthia Wong, DMD, MS
Program Director
University of Rochester
Rochester, New York, United States
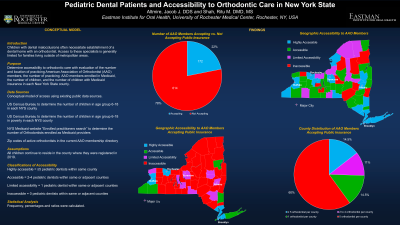
Pediatric Dental Patients and Accessibility to Orthodontic Care in New York State
Malocclusion has been mainly described as misaligned teeth, but it is a problem that can reduce social acceptability and affects the quality of life of a person1. Therefore, orthodontic treatment is important because it will guide the most appropriate facial development, improve self-esteem, function and esthetics. The high costs of orthodontic treatments prevent access to the general population, especially low-income families. Therefore, Medicaid programs, Title XIX of the social security act, was created to make dental care, including orthodontic treatments, available to this population2,3The main goal of these programs is to aid these populations by decreasing financial barriers and increasing their ability to be treated in the conventional health care system5. Now a days, all states offer some level of orthodontic coverage under Medicaid, but the number treated is a lesser fraction of the total population with orthodontic needs despite their eligibility to Medicaid4. Many orthodontists are hesitant to enroll as a Medicaid provider due to low reimbursementfrom the state, excessive bureaucracy and paperwork, difficult eligibility for treatment, difficulty collecting fees from Medicaid, delays in receiving payments, prior authorization requirements, potential for loss of coverage during treatment and the higher rate of noncompliance and failed appointments1,2,5,6.
Therefore, we propose to conduct a study to evaluate:
1. Accessibility to orthodontic care by evaluating the number of practicing orthodontists, the number of practicing orthodontists enrolled in Medicaid, the number of children, and the number of children with Medicaid insurance in each New York State county.
Data:
1. TBD
References:
1. Okunseri C, Pajewski N, McGinley E, Hoffmann R. Racial/Ethnic Disparities in Self-Reported Pediatric Orthodontic Visits in the United States. Am Assoc of Public Health Dent. 2007; 67 (4): 217-23
2. Theis J, Huang G, King G, Omnelld M. Eligibility for publicly funded orthodontic treatment determined by the handicapping labiolingual deviation index. Am J of Orthod and Dent Orthop. 2015;128:708-15
3. Salzmann, J A. Provision of orthodontic and general dental care under Medicaid in New York State. Am J of Orthod. 1967;53:618-9
4. Proffit WR, Fields HW, Moray LJ. Prevalence of malocclusion and orthodontic treatment need in the United States: estimates from the NHANES III survey. Int J Adult Orthodon Orthognath Surg. 1998;13(2):97-106.
5. Horsley B, Laindauer S, Bhavna S, Tufekci E, Abubaker AO, Fowler C, Maxfield B. Appointment keeping behavior of Medicaid vs non-Medicaid orthodontic patients. Am J of Orthod Dentofacial Orthop. 2007;132:49-53
6. Wilson J, Harris EF. Compliance by state-subsidized and self-pay orthodontic patients. Am J of Orthod Dentofacial Orthop. 2015;148:628-32