
.png)
Oral Pathology
Dan Bamshad, DDS
Resident
Cohen Children’s Medical Center of Long Island Jewish Hospital, Queens, NY
Cohen Children’s Medical Center of Long Island Jewish Hospital
Great Neck, New York, United States
Kathleen Schultz, DMD
Attending Doctor
Cohen Children's Medical Center, Queens NY
Queens, New York, United States
Paul Crespi, DDS
Program Director
Cohen Children's Medical Center, Queens NY
Queens, New York, United States
Kathleen Schultz, DMD
Attending Doctor
Cohen Children's Medical Center, Queens NY
Queens, New York, United States
Paul Crespi, DDS
Program Director
Cohen Children's Medical Center, Queens NY
Queens, New York, United States
A buccal bifurcation cyst/inflammatory buccal cyst is a rare inflammatory odontogenic cyst that typically occurs at the buccal region of the first or second mandibular molars at the time of eruption, although involvement of erupting premolars and third molars have been observed. This is typically found in children aged between 6-8 years and 11-12 years old, correlating with the eruption of the associated molar. Histologic examination is performed to rule out benign odontogenic cysts and tumors, and often reveals inflammatory epithelium consistent with an inflamed cyst, the buccal bifurcation cyst is identified by clinical, radiographic and histologic findings.
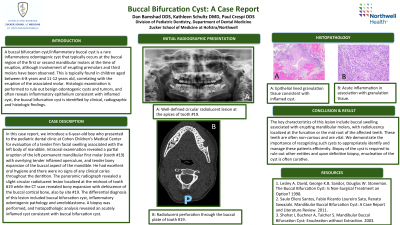
In this case report, we introduce a 6-year-old boy who presented to the pediatric dental clinic at Cohen Children’s Medical Center for evaluation of a tender firm facial swelling associated with the left body of mandible. Intraoral examination revealed a partial eruption of the left permanent mandibular first molar (tooth #19) with an overlying inflamed operculum, and tender bony expansion of the buccal aspect of the mandible. He had excellent oral hygiene and there were no signs of any clinical caries throughout the dentition. The panoramic radiograph revealed a slight circular radiolucent lesion localized at the mid-root of tooth #19 and the CT scan revealed bony expansion with dehiscence of the buccal cortical bone. The differential diagnosis of this lesion included buccal bifurcation cyst, inflammatory odontogenic pathology and ameloblastoma. An incisional biopsy was performed, and histopathologic analysis revealed an acutely inflamed cyst consistent with buccal bifurcation cyst. Management of the cyst included a subperiosteal exploration and enucleation.
This case report presents the diagnosis and treatment of a buccal bifurcation cyst with enucleation and curettage without extraction of the involved tooth. The key characteristics of this lesion include buccal swelling associated with erupting permanent mandibular molars, with radiolucency localized at the furcation or the mid-root of the affected teeth. These teeth are often non-carious and have vital pulpal tissue. Histologic examination was performed to rule out more concerning pathology and definitive treatment consisted of subperiosteal exploration and enucleation.