
.png)
Caries

Audrey Niemchick, DDS
Pediatric Dental Resident
Children's Hospital Colorado, Aurora, CO
Children's Hospital Colorado
Denver, Colorado, United States
.jpg "Katherine Chin, DDS photo")
Katherine Chin, DDS
Medical Director
Children's Hospital Colorado
University of Colorado
Aurora, Colorado, United States
Souha Fares, MS, PhD
University of Colorado
Tamanna Tiwari, MPH, MDS, BDS
University of Colorado Anschutz Medical Campus
Aurora, Colorado, United States
Tamanna Tiwari, MPH, MDS, BDS
University of Colorado Anschutz Medical Campus
Aurora, Colorado, United States
.jpg "Roopa P. Gandhi, BDS, MSD photo")
Roopa P. Gandhi, BDS, MSD
Residency Program Director
Children's Hospital Colorado
Aurora, Colorado, United States
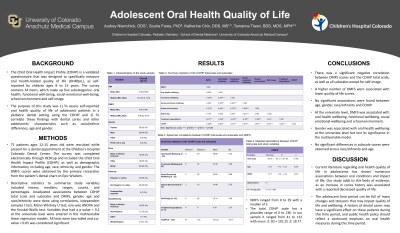
Purpose: The purpose of this study was to assess self-reported oral health quality of life of adolescent patients, and correlate these findings with dental caries.
Methods: A survey was collected electronically through REDCap from 74 patients ages 12-15 years old at the Pediatric Dental Center at Children’s Hospital Colorado. The survey consisted of demographic information, including age, race, ethnicity, and gender, and the Child Oral Health Impact Profile (COHIP). The DMFS scores were obtained by the primary researcher from the patient’s dental chart on Epic Wisdom. Descriptive statistics to summarize study variables included means, medians, ranges, counts, and percentages. Unadjusted associations between COHIP total scale and subscales and DMFS, gender, age and race/ethnicity were done using correlations, independent samples t test, Mann-Whitney U test, one-way ANOVA and the Kruskal-Wallis test. Variables that had a p-value < 0.2 at the univariate level were entered in the multivariable linear regression models. All tests were two-tailed and a p-value < 0.05 was considered significant.
Results: DMFS ranged from 0 to 29 with a median of 3. The total COHIP scale has a plausible range of 0 to 136. In our sample it ranged from 41 to 132 with mean ± SD = 101.25 ± 18.77. There was a significant negative correlation between DMFS scores and the COHIP total scale, as well as all subscales except for self-image. A higher number of DMFS were associated with lower quality of life scores. No significant associations were found between age, gender, race/ethnicity and COHIP. At the univariate level, DMFS was associated with oral health wellbeing, functional wellbeing, social emotional wellbeing and school environment. Gender was associated with oral health wellbeing at the univariate level but lost its significance in the multivariable model. No significant differences in subscale scores were observed across race/ethnicity and age.
Conclusions: Current literature regarding oral health quality of life in adolescents has shown numerous associations between oral conditions and impact of life. This cross-sectional study adds to this body of evidence, as an increase in caries history was associated with a reported decreased quality of life.