






- Pharmacology
- Allergy, Immunology, and ENT
- Cardiology
- Emergency Medicine
- Endocrinology
- Adolescent Medicine
- Gastroenterology
- Infectious Diseases
- Neurology
- OB/GYN
- Practice Improvement
- Gynecology
- Respiratory
- Dermatology
- Mental, Behavioral and Development Health
- Oncology
- Rheumatology
- Sexual Health
- Pain
Vision screening update: New device detects amblyopia and strabismus
Neural performance scanning (NPS) technology outperforms photoscreeners for analyzing binocularity in a child’s eyes in mere seconds, and with higher sensitivity and specificity.


Table 1
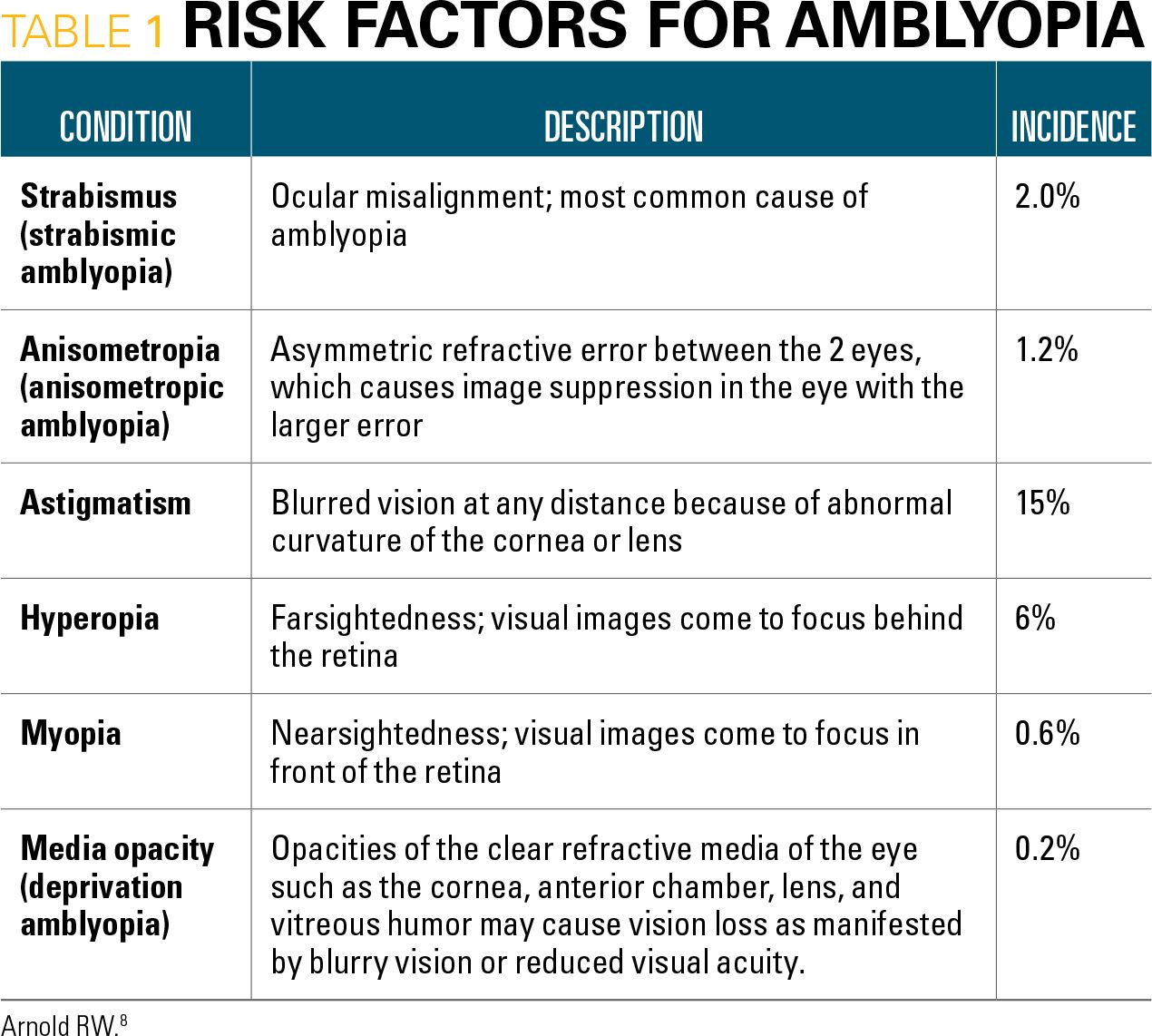


Table 2
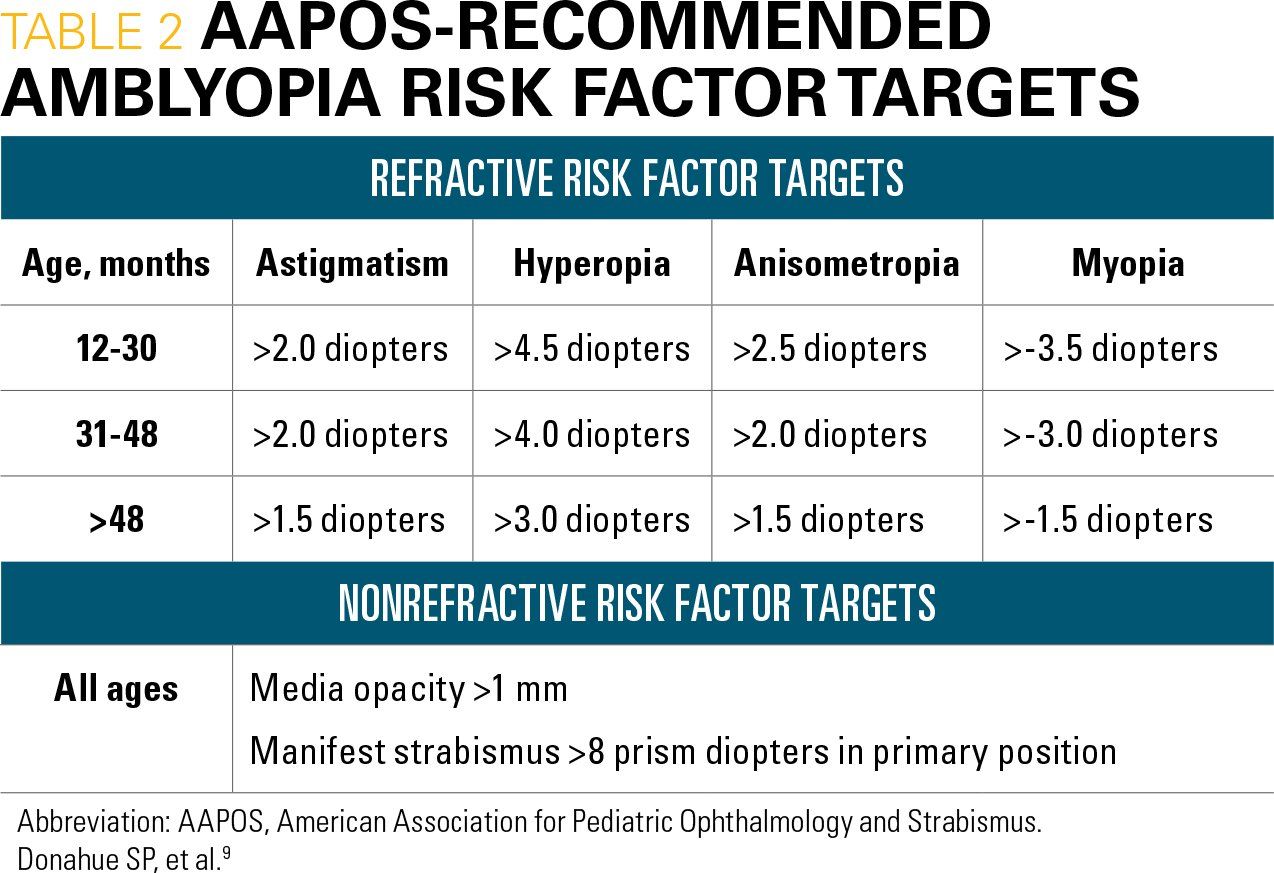


Figure 1
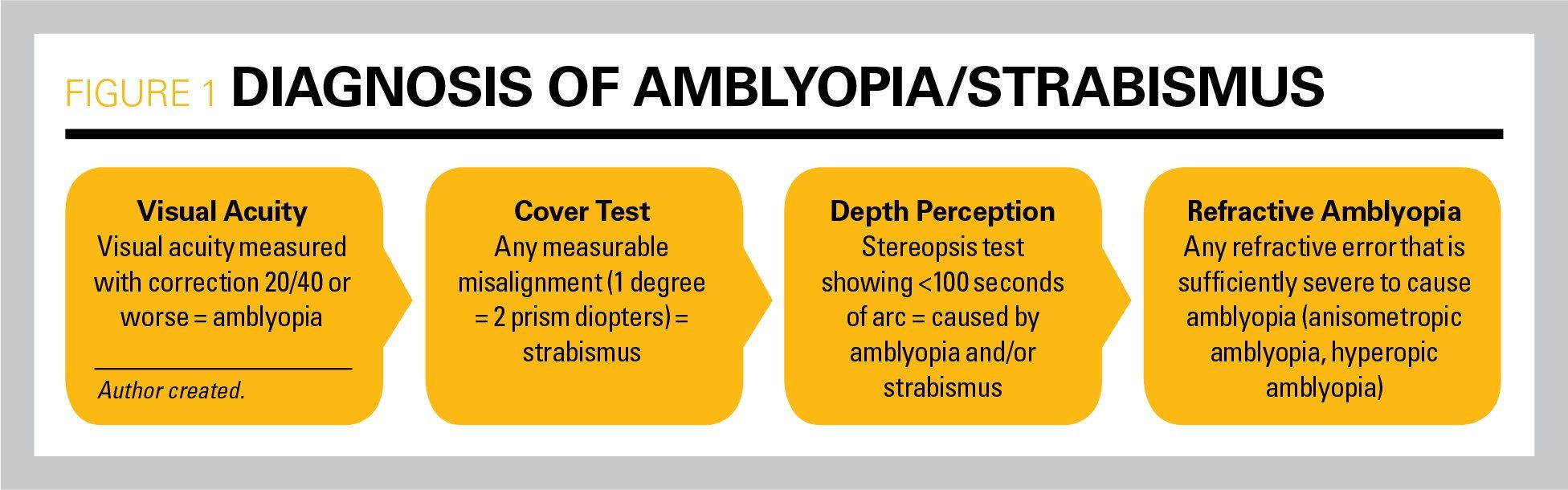


Figure 2
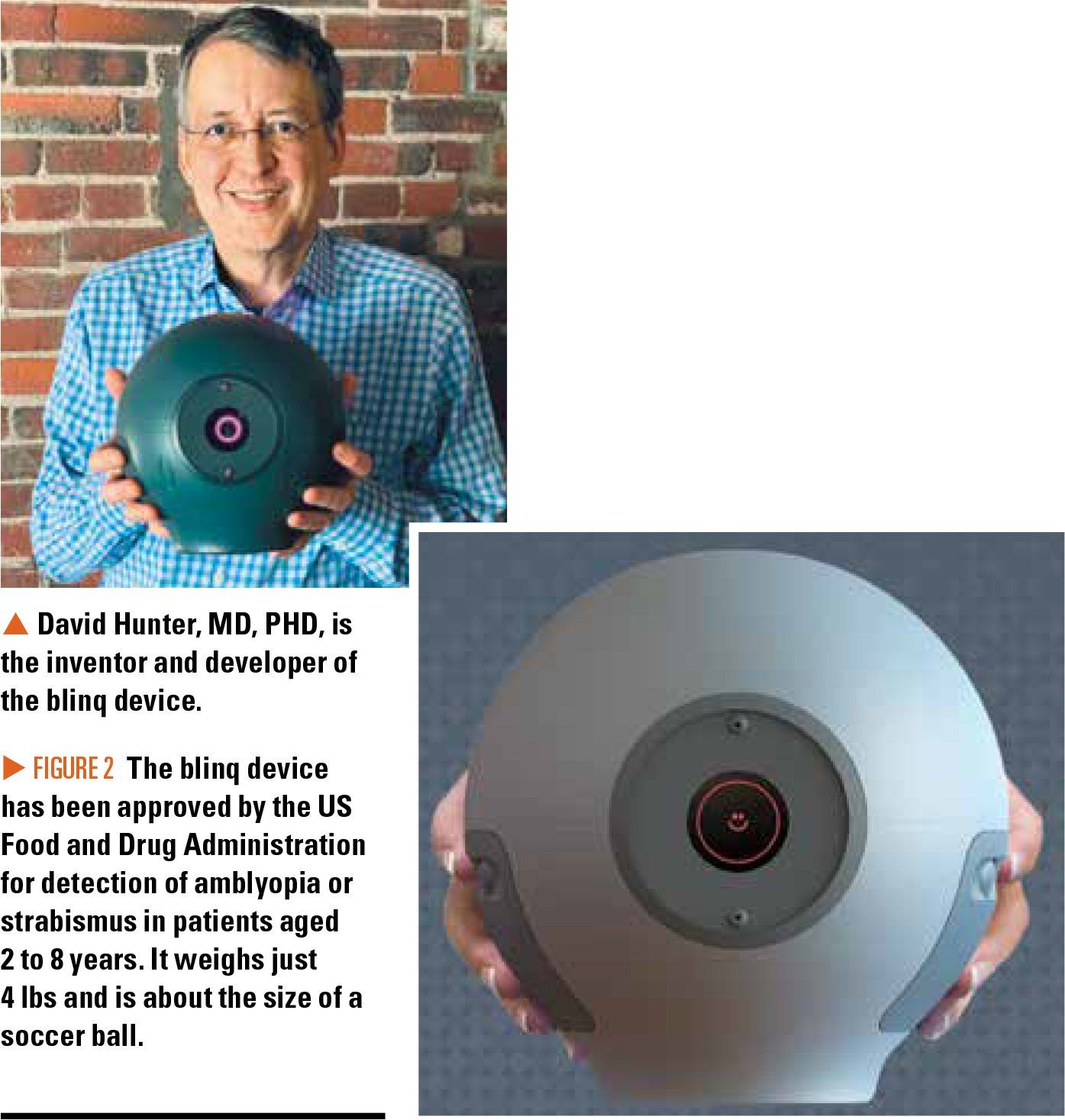


Figure 3
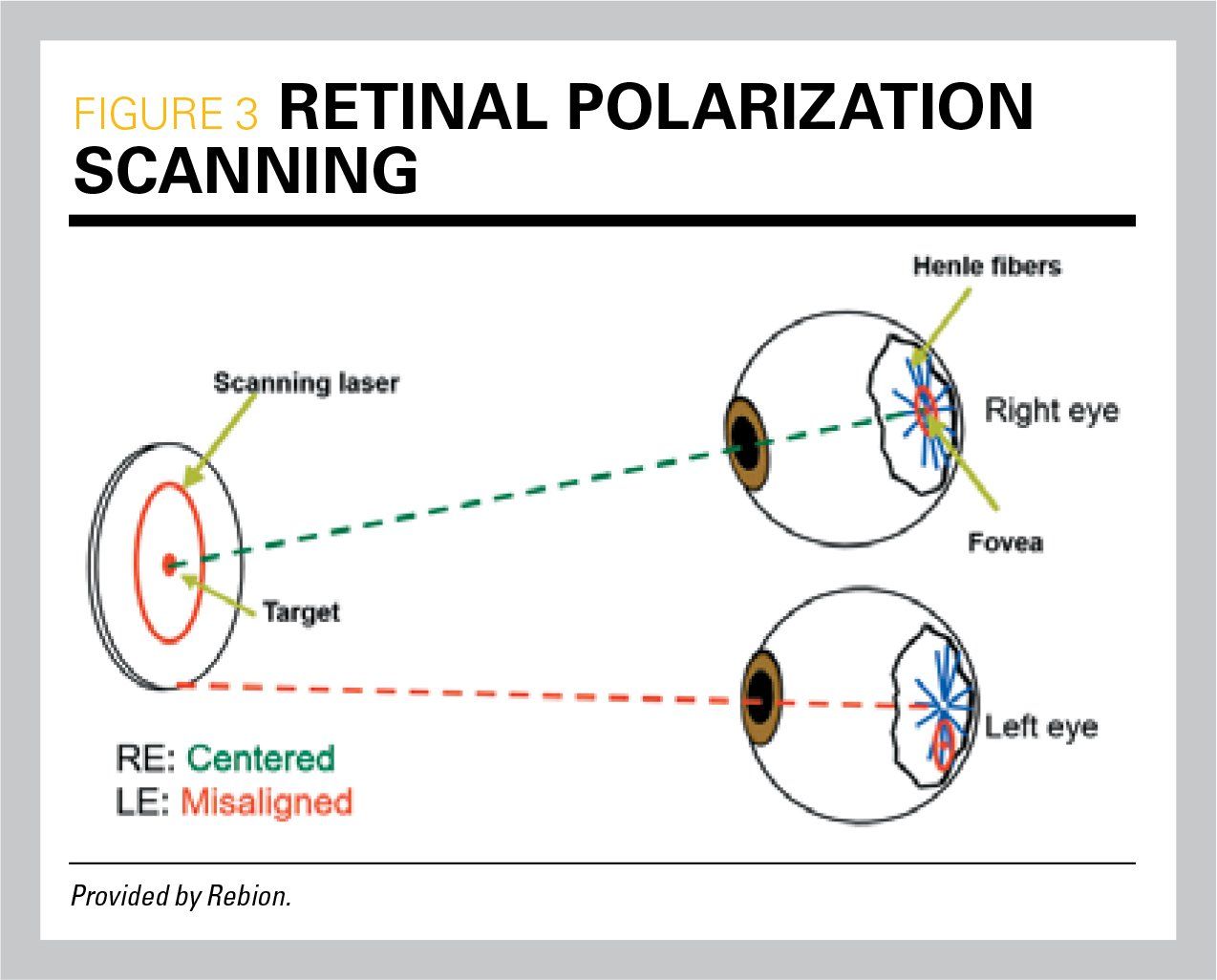


Figure 4
Editor's note: The products reviewed by Dr. Andrew Schuman are of his own selection and do not reflect the opinions of Contemporary Pediatrics or of the editors. He discloses no affiliation with any company mentioned in this article.
The American Academy of Pediatrics (AAP), the American Association for Pediatric Ophthalmology and Strabismus (AAPOS), the American Association of Certified Orthoptists, and the American Academy of Ophthalmology (AAO) last updated their guidelines on pediatric vision screening in 2016, after endorsing instrument-based vision screening 4 years earlier in 2012.1,2 Despite these recommendations, less than 40% of children have had their vision tested even once by age 5 years.3
I last reviewed instrument-based vision screening for Contemporary Pediatrics in February 2014. This update will review the importance of vision screening preschool children as well as introduce pediatricians to a new technology that will significantly improve the detection of amblyopia and strabismus in our patients.
Why screen for vision problems in children?
Approximately 2.5% of all children have amblyopia.4,5 Amblyopia is poor vision, typically in one eye, that occurs when the brain does not recognize the sight from that eye, even if the eye itself is structurally normal. Amblyopia responds best when detected and treated in the preschool years. If treatment does not start by age 7 years, amblyopia may never improve. Delayed detection of amblyopia leaves a child with permanent uncorrectable monocular vision loss that was potentially preventable. Children with amblyopia lack binocular vision and as a consequence are likely to suffer from poor school performance, reduced fine motor skills, and impaired self-esteem. Children with amblyopia are asymptomatic and remain undiagnosed and untreated unless they undergo vision screening.
Whom (and how) to vision screen
In theory, children can be screened for vision problems with traditional eye charts by the age of 3 to 5 years. Screening is possible with Snellen eye charts, Tumbling E vision charts, or picture tests such as Allen Visual Acuity Cards, but this is time consuming and can lead to inconsistent or erroneous results. In reality, however, visual acuity testing in children aged younger than 5 years in a medical office can be challenging, and few children this age can be screened with any type of vision chart.
Over the past 10 years, many pediatric practices have adopted instrument-based vision screeners, called photoscreeners, to identify children with amblyopia risk factors (ARFs) that predispose toward the development of amblyopia. These devices use an infrared camera that captures and analyzes images of the red ref lex of undilated pupils to screen for refractive error (hyperopia or myopia), astigmatism (warped lens), anisometropia (significant refractive difference between eyes), strabismus (eye misalignment) and lens opacity. (Please see my 2014 article for a detailed description of several photoscreeners-all the devices in that article are still on the market.) The advantage of photoscreeners is that little cooperation, and no verbal response, is required for testing, and the screening can be completed in less than a minute.
According to AAP guidelines, a visual acuity screen is recommended at ages 4 and 5 years, as well as in cooperative 3-year-olds. Additionally, instrument-based screening may be used for children aged 12 and 24 months, as well as for children aged 3 through 5 years. Visual acuity screening also should be performed by pediatricians at ages 6, 8, 10, 12, and 15 years and any time vision problems are suspected.6 The US Preventive Services Task Force (USPSTF) recommends that children undergo instrument-based vision screening at least once between the ages of 3 to 5 years.7
Amblyopia risk factor screening limitations
According to Robert Arnold, a pediatric ophthalmologist and co-author of the current AAPOS automated vision screening guidelines, ARFs are very common, with a mean combined prevalence of 21% compared with a prevalence of amblyopia (20/40 and worse) of 2.5%.8 By his estimates, the approximate prevalence of astigmatism is 15%, strabismus is 2.0%, hyperopia is 6%, myopia is 0.6 %, and anisometropia is 1.2% (Table 1).
Although photoscreening in pediatric practice has improved the number of children diagnosed with and treated for amblyopia, this technology has limitations and has not evolved since its introduction over a decade ago. Because the incidence of ARFs is 1 in 5 children, and the incidence of amblyopia is 1 in 40 children, only about 1 in the 8 children with risk factors who undergo a thorough examination by an ophthalmologist will be diagnosed with amblyopia.
In 2013, the AAPOS Vision Screening Committee revised its criteria for instrument-based vision screening because “many children, especially those having mild amblyopia, often have marked improvement (and sometimes even resolution) of their amblyopia with spectacle treatment alone; this phenomenon is seen in children with anisometropic amblyopia as well as those with strabismic amblyopia.” The committee noted that the referral criteria for photoscreening instruments should have high specificity for ARFs in young children (to minimize false-positive referrals) and high sensitivity for the detection of amblyopia risk factors in older children (when children are approaching an age when treatment becomes less effective).9 See Table 2 for the current age-related thresholds recommended by the AAPOS.
Additionally, many pediatricians and ophthalmologists report that only 38% to 48% of patients who are referred following photoscreening actually make appointments for follow up.10-12
So, to summarize, the current referral rate from photoscreening is too high (poor specificity for amblyopia detection) and compliance with referrals is so poor that many young children with amblyopia continue to go undiagnosed.
Amblyopia diagnosis and treatment
The most common cause of amblyopia in children aged 3 years and younger is strabismus, occurring in 82% of cases, whereas combined strabismus and anisometropia is the cause in approximately 13% of cases, with 5% resulting from anisometropia alone.13 In older children aged 3 to 6.9 years, strabismus or anisometropia each occur in 40% of cases, with about 20% of cases resulting from combined strabismus and anisometropia.14 Thus, many children with amblyopia may not have ARFs other than strabismus.
To confirm a diagnosis of amblyopia, an ophthalmologic exam is needed to perform the following: measure visual acuity; perform a cover test for strabismus; test depth perception (stereopsis); dilate the pupils (cycloplegia); perform a refraction; and examine the inside of the eye to confirm there is no structural eye disease (Figure 1). Although ophthalmologists and pediatricians both measure visual acuity, testing is more accurate when performed by ophthalmologists given the nature of their training and child-specific testing methods available to them.
The relationship between refractive error and the likelihood of amblyopia depends on the child’s age, severity of blurred vision, and other factors such as their ability to accommodate and their propensity for developing strabismus.9 For children aged 3 years and younger, the prevalence of amblyopia correlates with the severity of anisometropia.15 Many children with mild amblyopia from anisometropic amblyopia or strabismic amblyopia improve with eyeglass treatment alone.16 Treatment options for children in whom eyeglasses are not appropriate or are ineffective include patching the better-seeing eye or using atropine drops to blur vision in the better-seeing eye.
Early detection and treatment of strabismus (of any degree) is important even in children who don’t have amblyopia, because timely correction of strabismus with glasses or surgery can preserve or recover binocular vision (depth perception). Also, strabismus may lead to the development of amblyopia! This is particularly true of children with esotropic strabismus, less so with children with exotropic strabismus.
A new technology for amblyopia detection
David Hunter, MD, PhD, is the Ophthalmologist-in-Chief at Boston Children’s Hospital, Massachusetts. He has spent more than 15 years developing a new technology for detecting amblyopia and strabismus in young children. This technology is called retinal polarization scanning (RPS), and the prototype device using the technology was originally called the Pediatric Vision Scanner. He formed Rebion (formerly REBIScan) in 2009 to commercialize the device, and the final version, recently released, has been appropriately named “blinq.” (Figure 2). Hunter named the propriety technology behind the blinq “neural performance scanning (NPS)” to remind users that the screening device was developed to help detect amblyopia “which is a brain disease, not an eye disease.”
The technology is based on the fact that when one eye has diminished vision, the brain cannot align both eyes to achieve stable binocular fixation. When polarized light is projected on the nerve fibers surrounding the fovea (the area of the retina responsible for central vision), these fibers change the polarization of light projected onto this area. The blinq device projects a beam of polarized light onto the retina while the child focuses on a light target 14 inches away, and the changes from the light reflected by the fovea of each eye are analyzed by the device (Figure 3). Five scans are completed in a 2.5-second interval and the device calculates a binocularity score. A score above 60 indicates perfect eye alignment. A score below this measurement indicates amblyopia, strabismus, or microstrabismus.
The device can detect as little as 1 degree of strabismus. (In contrast, at least 8 degrees of strabismus must be present before it can be detected visually by a non-ophthalmologist.) Although photoscreeners provide a readout indicating that strabismus is present, they also require at least 8 degrees of strabismus, the same as what can be detected visually by parents or pediatricians. Independent comparative studies have shown excellent sensitivity (97%) and specificity (87%) of the blinq prototype for detection of amblyopia or strabismus.17-19 In short, the blinq detected all the conditions listed in Figure 1 with 97% sensitivity, in contrast with photoscreeners, which detect only refractive error and had only 74% sensitivity. Photoscreeners also resulted in a lower specificity, with a false referral rate of 38%.17
The blinq device is a grey orb with rubber handles on either side. It is roughly the size of a soccer ball and slightly heavier than the PlusoptiX 12C photoscreener that we use in our clinic. A touchscreen walks the user through the test sequence. One can enter patient information via the screen or via an online patient portal. One can also initiate a “quick” screen without inputting any information simply by pushing one of the buttons on either handle (my preferred method as this expedites screening). Testing is performed in an exam room with ambient lighting, or slightly dimmed lighting-bright lights are to be avoided.
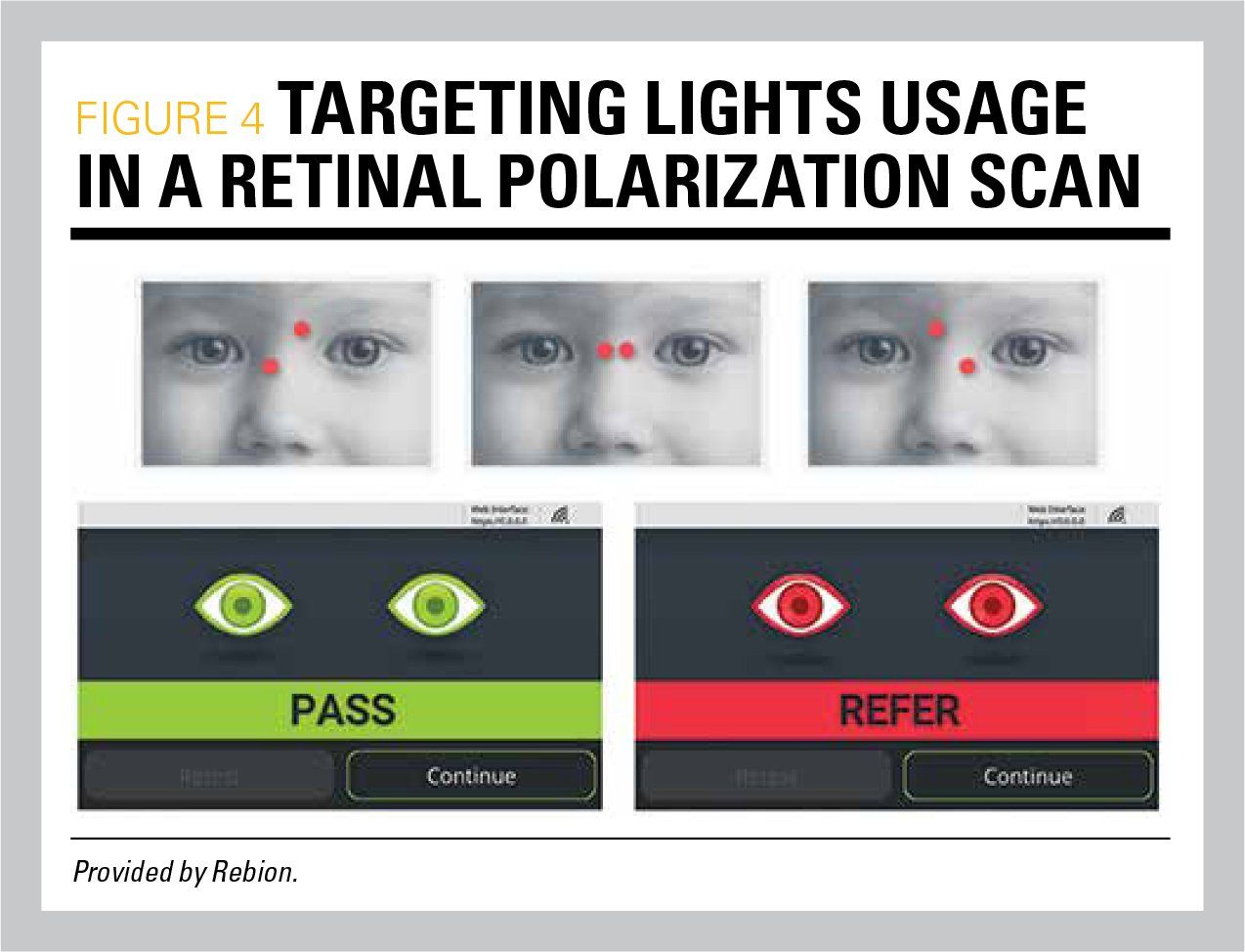
To begin a blinq screening, a tap of the scanning button will conduct a 1/10-second calibration. The child is then instructed to look at the lighted face image at the center of the orb and the examiner positions the 2 red targeting lights emitting from the device on the bridge of the nose, guiding blinq to/from the child to horizontally align the targeting lights. The device automatically performs 5 scans in a 2.5-second period, calculates a binocularity score, and displays a pass or refer result (Figure 4). If a patient is uncooperative, the testing sequence will time out in a preset time period that can be adjusted by the user-usually it is set at 10 seconds. As with all screening devices, only 1 successful screening result is necessary. If a time-out result occurs twice, then referral is recommended.
As of this writing, I have used the blinq device in my clinic for about a week and found it quite easy to hold and operate. As with any screening device, there is a “learning curve” until users achieve proficiency with testing. This was much the same when my clinic deployed routine photoscreening several years ago.
The blinq device weighs 4 lbs and has been approved by the US Food and Drug Administration (FDA) for use in patients aged from 2 to 8 years. The device operates on a rechargeable lithium battery, making it portable throughout the practice (clinic, exam room to exam room), but it also can be used with the charging cable attached. It has no direct printing capability but can connect via your practice’s wireless network to a cloud-based portal for storing information and printing results to a network-connected printer.
Rebion is working on integration for electronic health records (EHR) systems and this will be available in the near future with a software update. If you want to stay low tech regarding result documentation, Rebion provides a sample pack of prescription-sized result reporting pads to which you can affix patient labels, check the “pass” or “refer” box, and hand to your patient or scan into your EHR.
The device sells for $8995 and comes with a 1-year warranty. Rebion suggests users bill insurance companies using the CPT code 07X6T: “retinal polarization scan, ocular screening with on-site automated results bilateral.” By my estimates, if insurance companies reimburse $25 per test, the device will pay for itself after 360 screens, which for many practices can be easily achieved in 6 to 12 months’ time. It is possible that the test may be reimbursed at a higher rate.
We can do better
I said earlier that compliance of parents keeping appointments with pediatric ophthalmologists following referrals is below 50%. I have 2 suggestions to improve screening and follow-up rates. First, consider screening children overdue for screening exams whenever the opportunity arises (ie, screen at ill visits and not just at well-child exams). Secondly, I suggest that following a “refer” on a blinq screen, given its high accuracy, your practice makes an appointment with a pediatric ophthalmologist to ensure follow-up. Rebion is working on a “motivational” handout to educate parents regarding the importance of seeking a follow-up evaluation for diagnosis and treatment when indicated.
Also, be aware that the AAP has a Practice Improvement Module, called “Improve Preschool Vision Screening Performance Improvement Module,” that requires 3 cycles of 20 patient screens to complete. Upon completion, you can get 20 valuable Maintenance of Certification (MOC) part-4 credits for participation!
Lastly, in my opinion, practices would benefit from having both the blinq device and a traditional photoscreener. The blinq should be used in younger children to rule out amblyopia and strabismus, while photoscreeners can be used in older children at routine checkups, for those who have repeatedly passed a blinq screen every year through age 5. Photoscreeners used to screen patients at age 6 years and older can identify children with refractive errors and astigmatism that warrant referral to an eye professional. Photoscreeners used in this way will expedite vision testing in your office while improving workflow for well-child exams.
Retinal polarization scanning is an exciting new technology that has the potential for improving detection and treatment of the preschool child with amblyopia and strabismus. If you’d like to learn more, I’ve posted a review and discussion of the blinq device and technology on my Medgizmos.com website along with a webinar and an interview with the CEO of Rebion, Justin Shaka, and the inventor, David Hunter, as well.
References:
1. Donahue SP, Nixon CN; Section on Ophthalmology, American Academy of Pediatrics; Committee on Practice and Ambulatory Medicine, American Academy of Pediatrics; American Academy of Ophthalmology; American Association for Pediatric Ophthalmology and Strabismus; American Association of Certified Orthoptists. Visual system assessment in infants, children, and young adults by pediatricians. Pediatrics. 2016;137(1):29-30.
2. Miller JM, Lessin HR; American Academy of Pediatrics Section on Ophthalmology; Committee on Practice and Ambulatory Medicine; American Academy of Ophthalmology; American Association for Pediatric Ophthalmology and Strabismus; American Association of Certified Orthoptists. Instrument-based pediatric vision screening policy statement. Pediatrics. 2012;130(5):983-986.
3. National Health Interview Survey, CDC/NCHS. Data retrieved from Healthy People 2020 website. Available at: https://www.healthypeople.gov/2020/topics-objectives/topic/vision/objectives - 5373. Accessed April 2, 2019.
4. Friedman DS, Repka MX, Katz J, et al. Prevalence of amblyopia and strabismus in white and African American children aged 6 through 71 months the Baltimore Pediatric Eye Disease Study. Ophthalmology. 2009;116(11):2128-2134.e1-2.
5. Multi-ethnic Pediatric Eye Disease Study Group. Prevalence of amblyopia and strabismus in African American and Hispanic children ages 6 to 72 months the Multi-ethnic Pediatric Eye Disease Study. Ophthalmology. 2008;115(7):1229.e1-1236.e1.
6. Committee on Practice and Ambulatory Medicine; Bright Futures Periodicity Schedule Workgroup. 2019 recommendations for preventive pediatric health care. Pediatrics. 2019;143(3);e20183971.
7. US Preventive Services Task Force. Vision screening for children 1 to 5 years of age: US Preventive Services Task Force recommendation statement. Pediatrics. 2011;127(2)340-346.
8. Arnold RW. Amblyopia risk factor prevalence. J Pediatr Ophthalmol Strabismus. 2013;50(4):213-217.
9. Donahue SP, Arthur B, Neely DE, Arnold RW, Silbert D, Ruben JB; POS Vision Screening Committee. Guidelines for automated preschool vision screening: a 10-year, evidence-based update. J AAPOS. 2013:17(1):4-8.
10. Su Z, Marvin EK, Wang BQ, et al. Identifying barriers to follow-up eye care for children after failed vision screening in a primary care setting. J AAPOS. 2013;17(4):385-390.
11. Hered RW, Wood DL. Preschool vision screening in primary care pediatric practice. Public Health Rep. 2013;128(3):189-197.
12. Lowry EA, Wang W, Nyong’o O. Objective vision screening in 3-year-old children at a multispecialty practice. J AAPOS. 2015;19(1):16-20.
13. Birch EE, Holmes JM. The clinical profile of amblyopia in children younger than 3 years of age. J AAPOS. 2010; 14(6):494-497.
14. Pediatric Eye Disease Investigator Group. The clinical profile of moderate amblyopia in children younger than 7 years. Arch Ophthalmol. 2002;120(3):281-287.
15. Donahue SP. Relationship between anisometropia, patient age, and the development of amblyopia. Am J Ophthalmol. 2006;142(1):132-140.
16. Cotter SA; Pediatric Eye Disease Investigator Group. Edwards AR, Wallace DK, Beck RW, et al. Treatment of anisometropic amblyopia in children with refractive correction. Ophthalmology. 2006;113(6):895-903.
17. Jost RM, Yanni SE, Beauchamp CL, et al. Beyond screening for risk factors: objective detection of strabismus and amblyopia. JAMA Ophthalmol. 2014;132(7):814-820.
18. Loudon SE, Rook CA, Nassif DS, Piskun NV, Hunter DG. Rapid, high-accuracy detection of strabismus and amblyopia using the pediatric vision scanner. Invest Ophthalmol Vis Sci. 2011;52(8):5043-5048.
19. Jost RM, Stager D Jr, Dao L, Katz S, McDonald R, Birch EE. High specificity of the Pediatric Vision Scanner in a private pediatric primary care setting. J AAPOS. 2015;19(6):521-525.





















 | Image Credit: © woravut - © woravut- stock.adobe.com.")






